NURS 6050: Policy and Advocacy for Public Health Essays
NURS 6050: Policy and Advocacy for Public Health Essays
NURS 6050: Policy and Advocacy for Public Health Week 4 Discussion
Mental health is a public health issue worldwide. It spans across continents and affects many other aspects of a person’s health. According to Andersson et. Al (2014) “The World Health Organization estimates that depression will be the second most common disease leading to disability adjusted life years by 2020.” It is widely acknowledged that there is a disparity in the physical health of patients with and without mental illness Noblett and Henderson, 2015). Mental Health is not exclusive. It almost never exists without the presence of other health issues. It leads to the “chicken or egg first” type of debate. Mental health is influenced by all five population health determinants (medical care, individual behaviors, social environment, physical environment and genetics) in some manner but not proportionally.
CLICK HERE TO ORDER YOUR NURS6050 ASSIGNMENTS
Access to health care holds a symbiotic relationship to mental illness. S. Hardy et. Al (2012) found that significantly higher mortality rates from physical illness among those with a diagnosed mental illness, together with unequal access to health care had global significance when seen against wider health-inequality challenges. There are some mental health disorders such as Huntington’s that can only genetically linked. Others such as substance abuse, anxiety and depression have been shown to run in families. According to Web MD, it is referred to a genetic susceptibility. Genetics may pre dispose an individual to a mental illness but other factors or determinants may influence or trigger an illness in a person who has susceptibility to it. Many social behaviors affect the development of a mental health disease. Hardy and Thomas (2012) found that there is consistent evidence that suggests an unhealthy diet is a key modifiable risk factor for some mental health disorders.
Hardy et al. (2012) found that physical activity may not prevent depression, it has been shown to have a positive impact on mental health. Hardy et al (2012) discussed a relationship between increased poverty levels in England and increased diagnosis of mental health disorders amongst children in England. Other social factors may influence mental health disorders as well. For instance a occupation that offers mental health services leaders to timely and more effective interventions. Lower education levels may provide barriers to recognition and treatment of mental health disease. One’s physical state has a direct relationship on mental illness. Hardy et. Al states that a person with a mental health illness is nearly twice as more likely to have a serious health condition than the rest of the population. It is also commonly known that sunlight can have a positive affect on one’s mental health. This is why some health care providers may still use light therapy in the treatment of depression. Mental illness may be directly caused by genetics or may lead a person to be susceptible to mental illness. For instance, Huntington’s disease is a genetic disease. There is always a genetic link in development of the disease and can therefore, be prevented. Other mental health illness such al substance abuse, depression etc may lead a person susceptible to development but does not mean they will always develop the disease. I believe that all the determinants make an impact on mental illness in so………………………
NURS 6050: Policy and Advocacy for Public Health Essays – Discussion 1 (Walden)
MAIN QUESTION POST
The purpose of this discussion post explain how the United States government plays a role in health care and the Affordable Care Act. I will also take a stance on whether I believe …
With the recent enactment of the ACA, it is an easy question to ask, is health care a right or privilege? In my opinion, I believe that health care is a privilege and that it should be earned.
NURS 6050 Discussion 2 (Walden)
INITIAL POST
With the changes in the health care system, the demand for leadership in nursing is a priority. The transformation of nursing leadership is needed in all disciplines (National Academy of Sciences, 2011). The purpose of this discussion is to describe one of the research priorities that is of interest to me. I will explain the benefits and challenges of addressing this priority in nursing. Articles will be identified, and research will be presented on how this approach will support nursing leadership….
NURS 6050: Policy and Advocacy for Public Health Essays- Discussion 3 (Walden)
INITIAL POST
Health care policy decisions involve many concepts. Considering health policy decisions are health care costs, quality, and access (Laureate Education, 2012). The purpose of this discussion is to assess the ethical and economic challenges related to policy decisions when it comes to paying for expensive drugs and treatment. Explanations will be given on what contributes to the tension between cost of drugs and care. Sources will be added to my response….
NURS 6050 Discussion 4 (Walden)
Key Health Determinants
INITIAL POST
There are five determinants that influence health: Social, individual behaviors, genetics, physical environment, and access to health care (Kindig, Asada, & Booske, 2008). The topic of this discussion is to identify a population health issue of interest to me. I will explain and apply framework that is described in “A Population Health Framework for Setting National and State Health Goals”. Epidemiological information will be provided to support my information…
NURS 6050 Discussion 5 (Walden)
Thanks for the informative information regarding obesity in your county. I thought your county ratings were extremely high until I researched my county’s obesity ratings. I live in an….
NURS 6050: Policy and Advocacy for Public Health Essays – Discussion 9 (Walden)
The purpose of this discussion post is to evaluate an ethical scenario that encompasses a nurse caring for her sister’s HIV-positive boyfriend. I will post two resources that establish the nurse’s position. I will post my stance on the issue. I will determine whether the law and American Nurses Association (ANA)s standards support or conflict with the action…
NURS 6050 Week 10 Assignment (Walden)
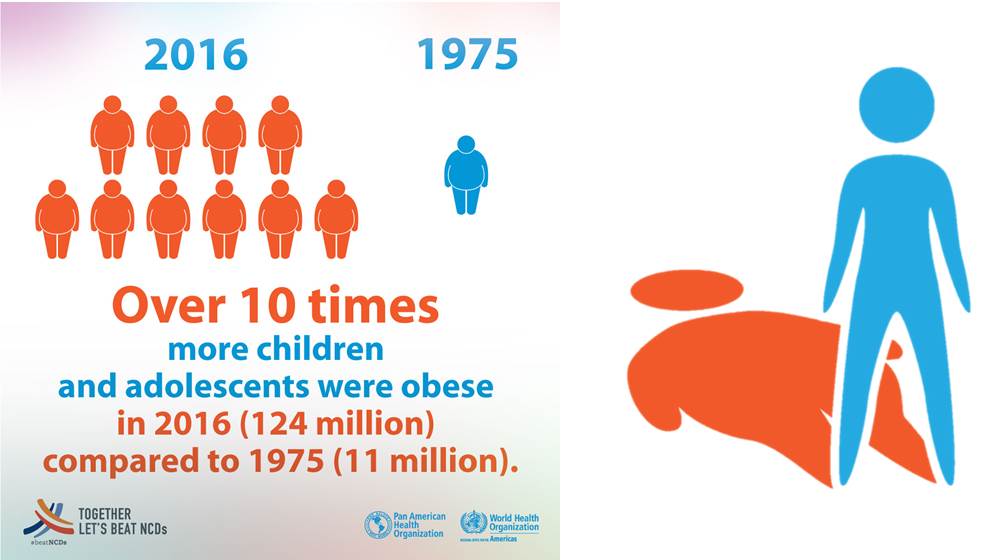
Defeating Childhood Obesity
NURS 6050 Policy and Advocacy for Population Health
Childhood obesity is a dangerous epidemic in the United States. According to the Centers for Disease Control and Prevention from 2011-2012 there were 12.7 million children and adolescents labeled as obese (Centers for Disease Control and Prevention [CDC], 2016)…
NURS 6050: Policy and Advocacy for Public Health Essays – Week 10 Discussion (Walden)
Main Post Question
Ethical Issues with an Aging Population
There are plenty of ethical challenges that nurses face when taking care of the older …
NURS 6050 Week 11 Discussion (Walden)
Global Nursing Issues
Global health issues are a concern for all people no matter what country they reside in. People in third world countries are dying or very ill from diseases that have been cured or …
Two Strategies for Challenges
Volunteering in third world countries is one to help with global health issues. Organizations must understand what motivates people to volunteer and continually give back to …
Advocating for Global Health
Nurses must be involved in policy decisions. A team of healthcare professionals can …
NURS 6050: Policy and Advocacy for Public Health Essays – Week 4 Assignment (Walden University)
Teenage Suicide: A Population Health Issue
Preview:
Teenage suicide is a topic that makes most people uncomfortable to discuss or think about due to the “loss of a life so young, and promising” as so often stated. According to the Centers for Disease Control and Prevention (CDC) suicide is the second leading cause of death between the ages of 10 to 24. The CDC also estimates for every teenager who takes their own life, there are about 50 more teenagers contemplating the act of suicide (Centers for Disease Control and Prevention, 2018)…..
NURS 6050: Policy and Advocacy for Improving Population Health “Population Health” Program Transcript
DR. PETER BEILENSON: Your zip code that you live in makes more difference in your health and well being than the genetic code that you’re born with.
NARRATOR: Doctor Peter Beilenson discusses the influence of social determinants on population health. And how epidemiologic data is used to identify population health problems. Doctor Beilenson shares examples from his experience as Baltimore City’s health commissioner.
[MUSIC PLAYING]
DR. PETER BEILENSON: The bottom line that we use all the time is place matters. The place that you grow up matters hugely. And if there’s a four legged stool of the things, of supports that allow for people to grow healthfully, and into decent social economic wellness, if you will– it’s access to health care. It’s access to decent education. To decent safe housing. And probably most importantly, access to livable wage paying jobs. It’s those four things that if you do you have them, you’re going to turn out much, much better in general than if you don’t have them.
CLICK HERE TO ORDER YOUR NURS6050 ASSIGNMENTS
I can give a perfect example of this in real life. Neighborhood in Baltimore called The Oliver Neighborhood. Which is a particularly decimated, vulnerable, under- served, left-behind neighborhood. It used to be very working-class African American. It’s now a drug infested area. There’s dilapidated housing with lead poisoned kids. There’s housing that has fallen down. The broken window theory of– once a couple of houses have broken windows, the neighborhood tends to go downhill because it looks like things aren’t being taken care of. And so more crime occurs. So it’s heavily crime infested.
There are a lot of the uninsured adults who don’t get their health care taken care of. So there’s a lot of chronic disease– diabetes, high blood pressure, strokes, et cetera. So there’s lack of decent housing, lack of health access. The schools that serve this neighborhood, Oliver, are particularly poor.
And lastly, not only is it a food desert in terms of not having good produce and fresh foods available because there are no supermarkets in the neighborhood. It’s literally a wage desert. I can’t think of any business in the Oliver neighborhood that pays a livable wage job.
So that’s a perfect crystallization of having nothing of the four legged stool of social determinants of health. Compare that with Howard County, Maryland. 12 miles away. Maybe three or four zip codes away. Where the vast majority of the population has access to great recreation facilities, excellent housing. There’s been one lead poisoned kid in the entire county of 300,000 people in the last couple of years, total. The percent of folks who are uninsured in that county is about 7% to 8%, 9%. Compared to 30% of the adults in this neighborhood in Baltimore.
The school system is ranked the best in the state. Probably one of the top 10 in the country. And there are innumerable living wage jobs. And, not surprisingly, the healthiest county in the state of Maryland is Howard county. And the poorest, the least healthy county in the city/county in the state of Maryland is Baltimore.
[MUSIC PLAYING]
DR. PETER BEILENSON: So the paradigm that the Institute of Medicine put out- – probably now it’s 15, 18 years ago. But it’s looking at health problems and health policy with a three step process. And epidemiology is particularly important in the first and third steps.
First step is doing a needs assessment of whatever population you’re serving. You assess the needs of the population that you’re serving. And that’s where epidemiology comes in. Statistics, data, et cetera. Depending on what issue you want to deal with. And when we picked priority areas when I was in Baltimore City, the Baltimore City Health Commissioner. We looked at areas that had large numbers of years of productive lives lost. Basically means if the average life expectancy is, let’s say 75 in the community, and something tends to kill people in their 30s, like AIDS did several years ago, that’s 40 something years of productive life lost. And so that’s an important thing to focus on.
Similarly, infant mortality. That’s 75 years of productive life lost. So the paradigm needs assessment can be done in looking at years of productive life lost. It can also be in a specific policy area like immunization. The needs assessment might be what part of your population is particularly un-immunized. And then go after that.
And then the second phase of this paradigm is policy development. So you assess the needs of your population. And to deal with them, you come up with policy. It could be legislation to address the issue that you’ve found. It can be a program that you start up. It can be advocating for change in a certain area to get that need addressed.
And the third component is assurance. Which is basically evaluation. We almost always in my work– whatever initiative that we launch– we always build in an evaluation tool at the end. So you can see if what you did, the policy you developed, met the need that you assessed.
© 2012 Laureate Education, Inc. 2
There are three classic examples that I’ve worked on in the last 15 years or so that highlight the use of this paradigm that The Institute of Medicine uses in terms of looking at ways to look at public health problems. Of needs assessment, policy development, and assurance. NURS 6050: Policy and Advocacy for Improving Population Health Essays
And the first is the immunization issue. In the mid to late 1990s– 1996 ’97 to be exact– we had worked with the Agency for International Development. At that time Vice President Al Gore wanted to choose an American city to show that the lessons that were learned outside our borders by the AID could be brought to bear on third world parts of the United States. And we were chosen first, here in Baltimore.
So the vice president came, along with the mayor and myself. And we went around a lot of vulnerable areas. And he was talking about some of the success stories that AID had had internationally.
And one of them was that the immunization rate in several impoverished developing countries, including Kenya, were significantly better than the immunization rates we had in our schools here in Baltimore. Even though there is a law that requires kids to be fully immunized before they go to school. It just wasn’t being enforced. Only 62% of kids in the school system were fully immunized or have records there of.
So the policy that we developed was multi-pronged. One of which was to do a lot of public relations communication to parents saying, hey we’re going to be dealing with this. We’re going to start holding you responsible. We had huge clinics in the school system buildings prior to school starting in the ’96- 97 school year. Where we had thousands and thousands of kids coming in to get immunized. And by the way, at the same time, not just school aged kids but their little siblings. So we hoped it would make a difference for kids coming up.
So we instituted these two policies. Again, this is something we could do ourselves. It was both communications based as well as offering services. And we went from 62% of kids at the beginning of that school year to 99.8% immunized within three months. And because we enforced this– so we went from something like 40,000 of the 100,000 kids unimmunized at the beginning to about 200. And as far as we could tell, from a lot of heavy work, most of those 200 actually moved out– they just were incorrect information that school system had about them. They actually weren’t even in the school system anymore.
So we basically went from one of the worst immunized cities in the country to one of the very best. And it stayed that way for the last 12, 14 years because the enforcement tools have been kept in place.
So needs assessment– in this case pretty simple. You just look at the data from the school system that show we were very under-immunized. Policy development, communications, legal ramifications. And offering clinics to immunize kids.
And assurance, following up to make sure that the law was enforced. That the rules were enforced at the schools system level. And keeping track of the kids going forward that were immunized. So a good public health success story. And a little bit unusual in that most public health problems, from AIDS to chronic disease, take decades to develop. And usually take a while to fix. In this case it took a decade to develop, but it took three months to fix.
Early 1998 the CDC– the Center for Disease Control and Prevention– comes out with their national rankings on syphilis. And Baltimore not only ranks first in the country, but we have one of every 20 cases in the entire United States in Baltimore City. You’ve got to assess what’s the epidemiology behind this outbreak. And it was very interesting. We actually, by the way, had hit the trifecta of being number one the country not only in syphilis but gonorrhea and chlamydia, too. Obviously, you would think somewhat related, but in reality not.
And that was because gonorrhea and chlamydia we’re tending to hit 13 to 25- year-olds if you looked at the data. Serially monogamous, which many nurses know, especially if you’ve taken care of teens. Serially monogamous means basically– you’re talking to the teenager, how many partners you have? One. How many partners in the last seven weeks? Five. Well you’ve been serially monogamous. But they tend to know their partner. And so it’s easy enough to do contact tracing. And to get the partners notified and medicated so that you can deal with the gonorrhea chlamydia outbreak. And so that was being done a lot through the school system and through our family planning clinics for teens.
Syphilis, when you looked at the data, was very, very different. It was 25 or older. More like 30 to 50-year-olds. Who were involved in drugs for sex, particularly crack. And were in crack houses and barely knew the person’s first name, if that. And so it was much harder to track and much harder to deal with. And looking at the epidemiology of it actually looked like it was sort of dispersed around the city. Which was surprising. But if you followed Baltimore’s history you knew that the year before a lot of the high rises that were disastrous, that concentrating a lot of impoverished drug-using population were torn down. And so they sort of shredded the populous and placed them all over the place. And so that was actually, we think, part of the reason for the spread. Because it wasn’t concentrated in one, or two, or three, or four places. But was all over the place. And so your chances of coming in contact with someone with syphilis was greater.
And once enough of the population, particularly the drug using population, of that age were infected then you’ve reached a tipping point whereby which you’re more likely to come in contact with someone who’s infected and therefore get infected yourself.
© 2012 Laureate Education, Inc. 4
So the policy we develop was a multi-pronged again. Partly was communication. So we wanted patients, or individual citizens, as well as providers, doctors and nurses, to know the signs and symptoms of syphilis. Because it was actually relatively rare before. And so we were seeing a lot of patients coming in from emergency rooms who had been treated for fungus. When actually they didn’t have a fungal infection, they clearly had syphilis. But the doctor or nurse practitioner had not seen a syphilis patient ever. And so they were misdiagnosing.
And so we actually encouraged people to send folks with genital lesions to our STD clinics. Because just as with heart bypass, the more you do, the more you know. The more you see, the better you are at treating it. So we did that. We actually trained our disease trackers in blood drawing. And sent them out. We didn’t do this terribly much, but we sent them out to crack houses to draw blood. Why? Because that’s where you do syphilis testing. And then we would come back and either shoot people up with penicillin there or bring them back to our clinics.
And then the third thing we did which was actually the biggest yield was– if you think about it– because they’re involved in the sex for drugs trade, a significant portion of this population is going to some way get arrested during a given year. Either for possession charges, or distribution charges, or prostitution charges, or whatever. And so we did STAT testing for syphilis at the central booking center. Which is where everybody comes in who gets arrested in Baltimore. And we had a huge yield of syphilis positive individuals.
And so they were at least– although you’re supposed to get three shots of penicillin– they at least got one before they were released within a day or two or three. And then we tried to follow up with many of them. But one shot at least makes a difference.
So within a year we had an 82.4% drop in our syphilis cases from 660 to something like low hundreds, mid hundreds. And it has stayed at or below that level virtually the entire time since. Because we’ve done a lot of outreach and are making sure that people who are in vulnerable populations are tested. We’re still too high. But we dropped out of the trifecta. And we are no longer number one in gonorrhea, chlamydia, or syphilis. And so it’s a significant success story. Although certainly we did not eliminate syphilis.